Is lack of evidence holding back advocacy services?
For Advocacy Awareness Week 2023, Fergus Hamilton and Tanyah Hameed from Social Finance explore whether independent advocacy services are held back by lack of evidence.
Independent advocacy can play a powerful role in helping people with learning disabilities and autistic people participate in decisions around important issues that affect their lives. At the same time, a general lack of data and evidence of impact are holding back advocacy organisations from making a collective case for funding and policy change in unstable funding environments.
To help bridge this evidence gap, The Henry Smith Charity has provided a three-year £2.6m grant to 15 advocacy organisations across the UK providing non-statutory advocacy and promoting self-advocacy groups. Part of the funding is allocated to Social Finance UK to work with organisations as a learning partner to:
- Better understand the nature of statutory versus non-statutory advocacy
- Profile the needs of those receiving advocacy support
- Convene learning partnership sessions with the organisations to support learning
- Develop an evidence-base for existing advocacy services
- Generate recommendations to support future funding and policy changes
In this article, we share some recent research findings from our ongoing work as part of this programme. We focus on why non-statutory advocacy is important, how it supports people, and areas where it can do more.
How do non-statutory advocacy services aim to make a difference?
Many of the grantee organisations on The Henry Smith Charity programme have described successful non-statutory advocacy as helping people to have a ‘voice’ and exercise their rights across a wide range of issues where they are not entitled to statutory advocacy support.[1]
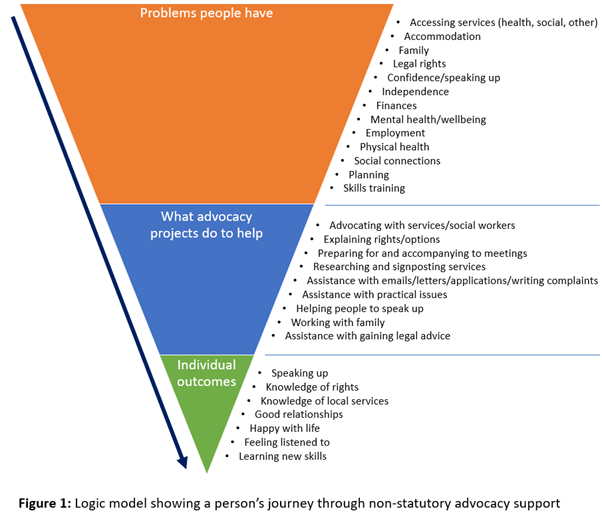
Operating broad eligibility criteria, grantees on the programme describe being entirely person-led in the issues they support people with. Individual goals can range from accessing health and social services to developing independent travel skills and better social connections. Through a combination of primary and secondary research, Social Finance identified the most frequent issues that people supported by these non-statutory organisations need help with, how they are supported by advocacy services and some of the key outcomes that might result.
Interviews and case studies of people using grantee services and self-advocacy groups revealed that people value the high degree of flexibility and responsiveness to individual needs and preferences that characterise the advocacy received through the organisations participating in the programme. This is rarely found in support received from social services, according to people we interviewed. This person-centred approach that allows non-statutory advocacy organisations to build trust among people whose past negative interactions with health and social services makes them difficult to reach.
How do non-statutory advocacy services support people and what are the outcomes?
In our latest phase of research, we wanted to better understand the nature of support people receive throughout their advocacy journeys. We have learned that grantees vary in the types of support they provide – some support self-advocacy groups, others specialise in one-to-one support, and some use a combination of self-advocacy and one-to-one support.
Some grantees provide general advocacy across a wide range of issues, support often spanning more than one issue category in cases where people require support with multiple goals. Other grantees specialise in working with specific groups in clearly defined circumstances, such as children with complex needs or parents with learning disabilities undergoing child protection procedures.
Through a process of data coding performed on qualitative data submitted biannually by grantee organisations, we identified nine distinct advocacy activity categories (see diagram above). Support is tailored to the goals of individuals and will typically involve a blend of advocacy activities as goals change and new goals and issues emerge as a case progresses.
Although the programme is still at an early stage, a comparison of start and end participant process outcomes data shows that non-statutory advocacy is having a positive impact on people who have received support. Process outcomes include things like ‘speaking up’, ‘knowledge of rights’, ‘good relationships’ and ‘learning new skills.’ We saw the largest positive changes in the ‘feeling listened to’ and ‘knowledge of local services’ categories, both of which relate strongly to some of the key aims and support areas for grantees.
As the programme progresses, we will continue to gather process outcome data to quantify the impact of advocacy on individual lives. We hope that this data can be used more widely to strengthen the argument for more sustainable funding for non-statutory advocacy, both for grantees and across the sector.
How can non-statutory advocacy services do more to support people and address issues of race equity?
Emerging findings from our research show that while non-statutory advocacy adds value and is an important part of the advocacy landscape in the UK, it may not be reaching some highly vulnerable groups. These groups include people with neurodegenerative conditions, older people in care homes, and ethnic minorities. While limited resourcing and funding are valid constraints, we feel that services could be more ambitious in trying to reach these groups – in particular vulnerable people from minority ethnic backgrounds.
Digging a bit deeper, our analysis showed that Asian ethnicities are underrepresented among those receiving support through The Henry Smith Charity programme, and we heard that this is reflective of wider challenges in this space. This may be for several reasons, including language and cultural barriers, a persisting stigma associated with learning disabilities in some Asian communities or a lack of awareness of advocacy and how it can help. Grantees also lacked detailed local data on ethnic minorities who have learning disabilities or are autistic, limiting their ability to understand who they were not reaching.
While issues of race equity cannot be solved overnight, we feel that there are some ‘quick wins’ that advocacy organisations can work toward. More inclusive recruitment to diversify staff, community events and translated posters to expand outreach, and sharing of testimonials and stories to boost word-of-mouth referrals are all potentially helpful ways to get started.
Affordable translation and interpretation services can also play an important part in overcoming linguistic barriers, especially in areas of high ethnic diversity. Funding and resourcing are perennial issues here, and addressing these gaps will not be easy. By demonstrating both the degree of need and the potential effectiveness of services through this programme, we hope to equip grantees with the evidence base to make a robust case for additional funding in the future.
Strengthening the case for sustainable funding
Our research so far is demonstrating that achieving outcomes related to the issue categories addressed by non-statutory advocacy can positively impact a person's life, building confidence, independence and overall wellbeing. This in turn has the potential to improve long-term physical and mental health outcomes that potentially reduce pressure on overburdened health and social care services.
In the second stage of the programme, we will focus on strengthening our growing impact evidence base through our outcomes framework. In the final stage, we will endeavour to build a robust case for funding by demonstrating potential commissioner savings accruing as a result of the powerful work being carried out by the grantees and non-statutory advocacy around the UK.
[1] Local authorities have a duty to ensure that statutory advocacy is provided to people treated under the Mental Health Act 1983, Mental Capacity Act 2005, Children Act 1989 and Care Act 2014.